Surgical instruments number in the thousands across all specialties, but the vast majority encountered in general surgery fall into five functional groups: instruments for cutting and dissection, instruments for grasping and holding, instruments for haemostasis, instruments for retraction, and instruments for suturing and tissue approximation. Understanding function before name makes the instrument trolley immediately logical rather than bewildering.
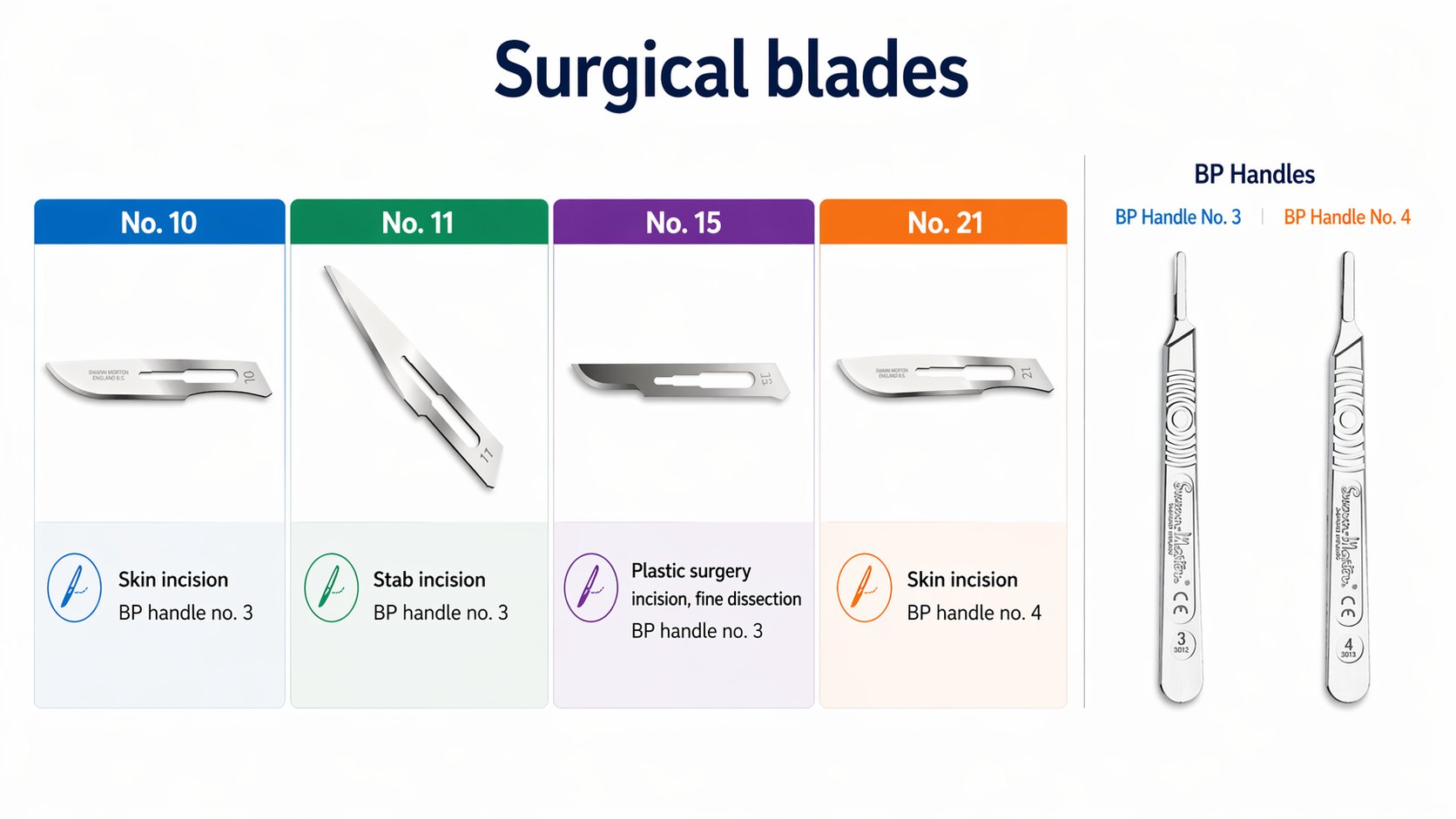
The scalpel consists of two components: the Bard-Parker (BP) handle and the detachable surgical blade. Handles are numbered by size. Handle number 3 is the most common and accepts blades 10, 11, and 15. Handle number 4 is heavier and accepts the larger blades 20 and 21, used for deeper or more robust incisions. Handles 7 and 9 are fine, elongated versions of number 3, used for delicate work in confined spaces.
| Blade | Profile | Use |
|---|---|---|
| No. 10 | Large curved belly | Standard skin incision in laparotomy and large wounds |
| No. 11 | Pointed, triangular | Stab incisions: draining abscesses, entering vessels, opening joints |
| No. 15 | Small curved belly | Fine dissection, plastic surgery, paediatric incisions |
| No. 20/21 | Large, heavy | Deep incisions through thick tissue, requires BP handle 4 |
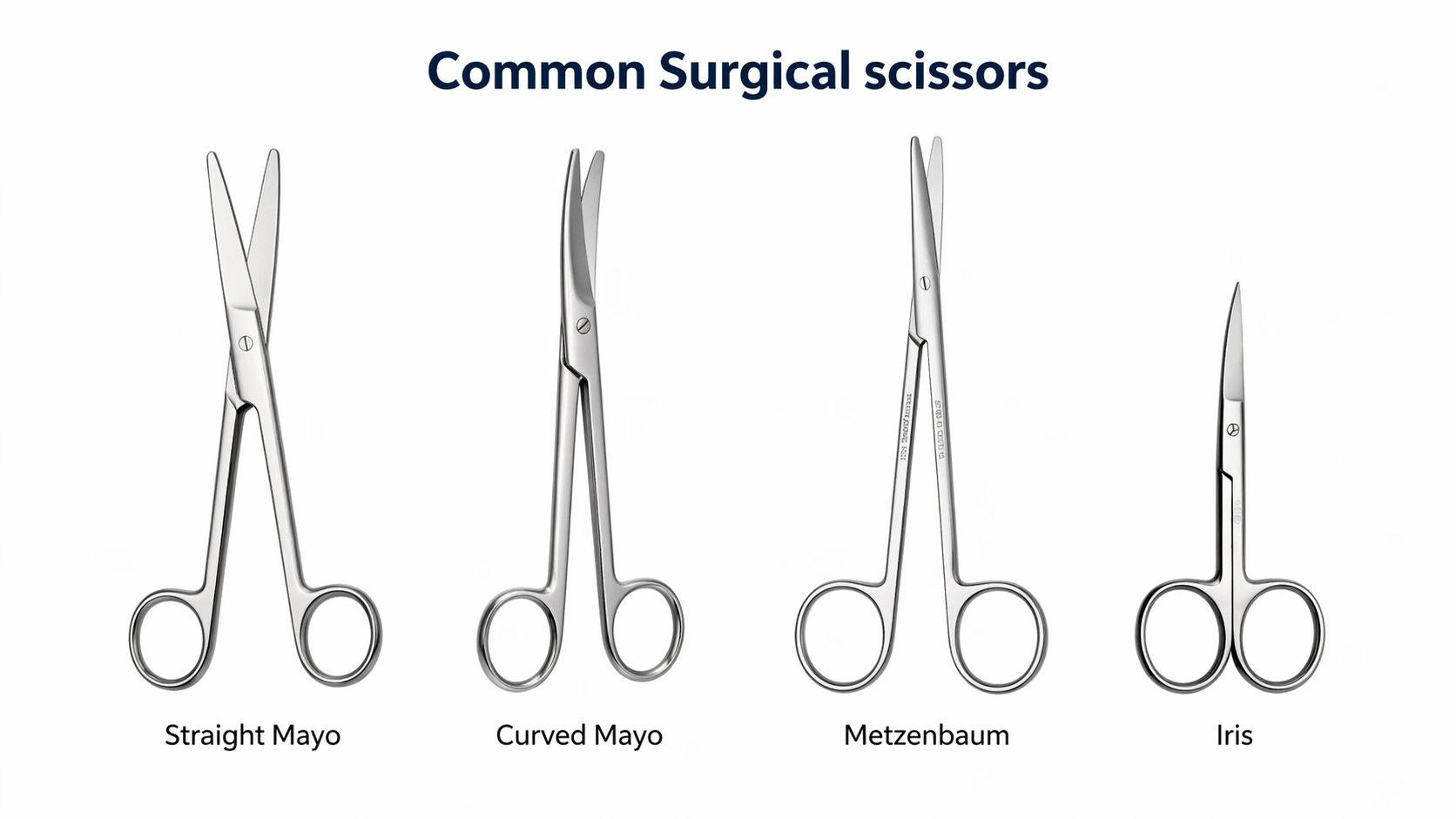
Surgical scissors serve two distinct purposes: tissue cutting and suture cutting. Using tissue scissors to cut sutures blunts them rapidly, and using suture scissors on tissue is poor technique. Keep the distinction clear from your first day in theatre.
Mayo scissors are the heavy workhorses. Straight Mayo scissors cut tough tissue and fascia, and are also used to cut sutures when a dedicated suture scissor is not available. Curved Mayo scissors cut through thick or deep tissue where the curve improves access and visibility.
Metzenbaum scissors (universally called 'Metz' in theatre) are lighter, longer, and designed for delicate tissue dissection. They are used in blunt dissection by gently opening the closed blades in a tissue plane, and in sharp dissection of fine structures. Never use Metz scissors to cut sutures: the blades are too fine and will be permanently damaged.
Iris scissors are small, fine-bladed scissors originally designed for ophthalmic surgery but now used for fine dissection and cutting fine sutures in any specialty. Potts scissors have angled tips and are used specifically to open blood vessels during vascular procedures.
Forceps, also called thumb forceps or pick-ups, are sprung non-locking instruments held between thumb and fingers and used to grasp, steady, or manipulate tissue. The choice between toothed and non-toothed tips is the critical decision.
Adson toothed forceps have a single tooth on one tip that interlocks with two teeth on the other. They provide secure grip on skin and subcutaneous tissue and are the standard instrument for skin closure. The teeth are traumatic to delicate tissue and must never be used on bowel, vessels, or nerves.
DeBakey forceps have fine longitudinal serrations on the tips but no teeth, providing grip without crushing. They are the default atraumatic forceps for vascular work and delicate dissection. If in doubt about which forceps to use, DeBakey forceps are almost always appropriate.
Bonney forceps are heavy toothed forceps with broad tips, designed for grasping thick tissue such as fascia during abdominal closure. Non-toothed tissue forceps (plain pick-ups) have serrated but toothless tips and are used for handling delicate structures where DeBakey forceps are not available.

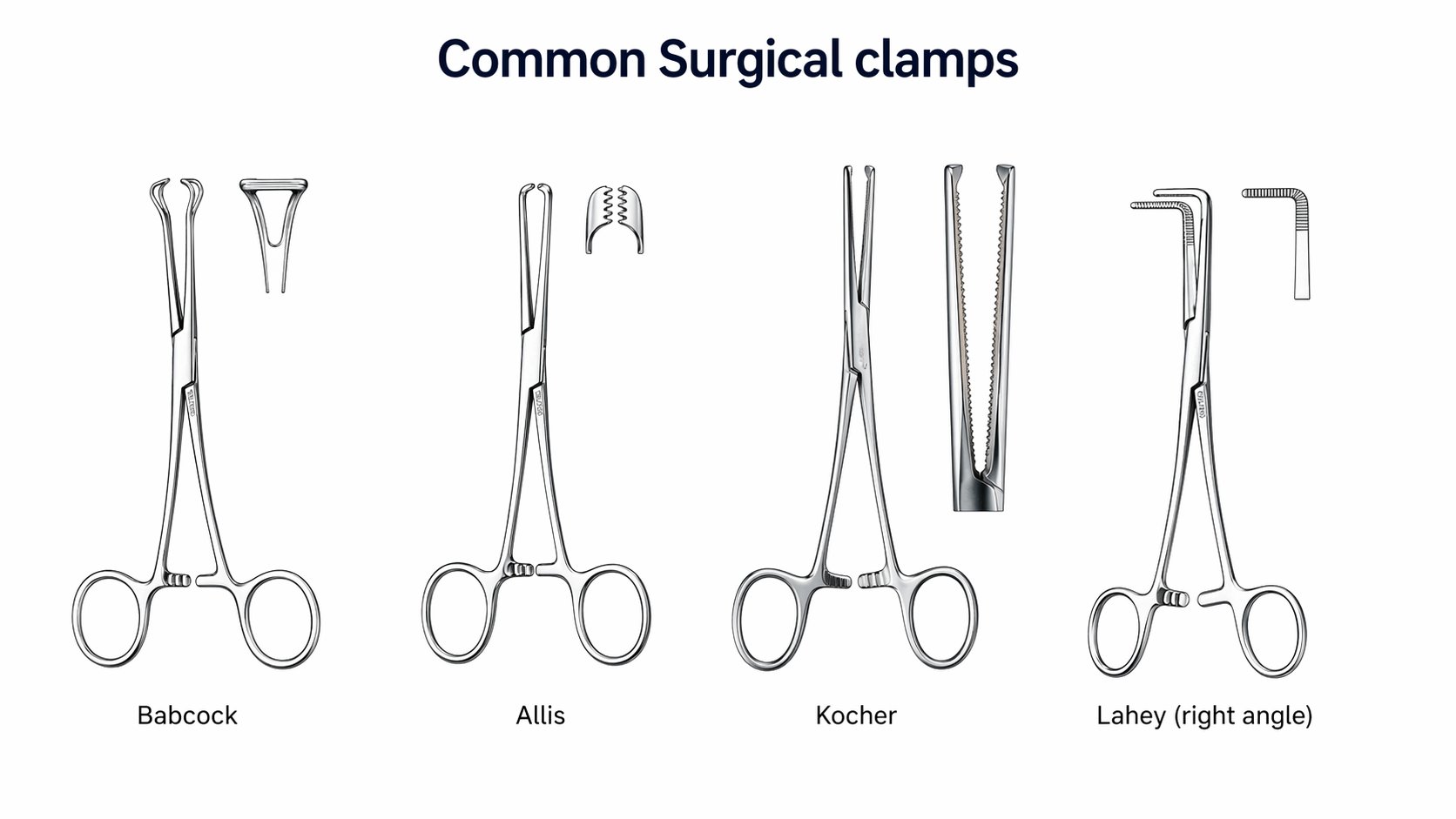
Clamps are ratcheted instruments that lock onto tissue and hold it without requiring the operator to maintain grip. They are classified as traumatic or atraumatic based on their jaw design.
Babcock clamp is the most commonly used atraumatic bowel clamp. Its triangular fenestrated jaws encircle rather than crush the tissue, making it safe for holding bowel, appendix, ureter, and bladder. It should encircle the structure, not compress it.
Allis clamp has fine interlocking teeth at the tip. It is traumatic and suitable only for tough tissues such as fascia, fibrous tissue, and flap edges. It is never used on bowel, skin, or vessels.
Kocher clamp (also called a crushing clamp or Kocher's forceps) has a transverse serrated blade with a terminal tooth. It is a traumatic instrument designed to hold tissue that will be removed or ligated. Used to clamp deep bleeding vessels and hold fascial edges.
Rampley's sponge-holding forceps (also called swab holders) have looped, ringed tips used to hold gauze swabs for skin preparation and for swabbing cavities. They are also used to hold the gallbladder, stomach, and cervix.
Lahey forceps (right-angled forceps) have a 90-degree curve at the tip and are used for dissecting around structures before ligation, particularly vascular pedicles and bile ducts. They allow a ligature to be passed around a vessel in a confined space without direct visualisation of the deep surface.
Haemostatic clamps are ratcheted, serrated-jaw instruments used to occlude bleeding vessels before ligation or diathermy. They are available straight or curved. The curved variety is most common because the curve aids visualisation of the vessel tip for tying.
Mosquito forceps (Halsted's mosquito) are the smallest haemostatic clamps, used for tiny vessels in superficial tissue. Crile forceps are slightly larger and widely used in general surgery for vessels up to approximately 3 mm. Kelly forceps are larger still, with serrations on only the distal half of the jaw. Roberts artery forceps are longer and heavier, suitable for deeper vessels.
The Spencer Wells forceps, widely used in gynaecological and obstetric surgery, have strong rigid teeth that improve grip and compression on arterial vessels. Kocher's forceps, although classified as a clamp, also serve a haemostatic role in deep bleeding vessels where a standard artery forceps cannot reach.
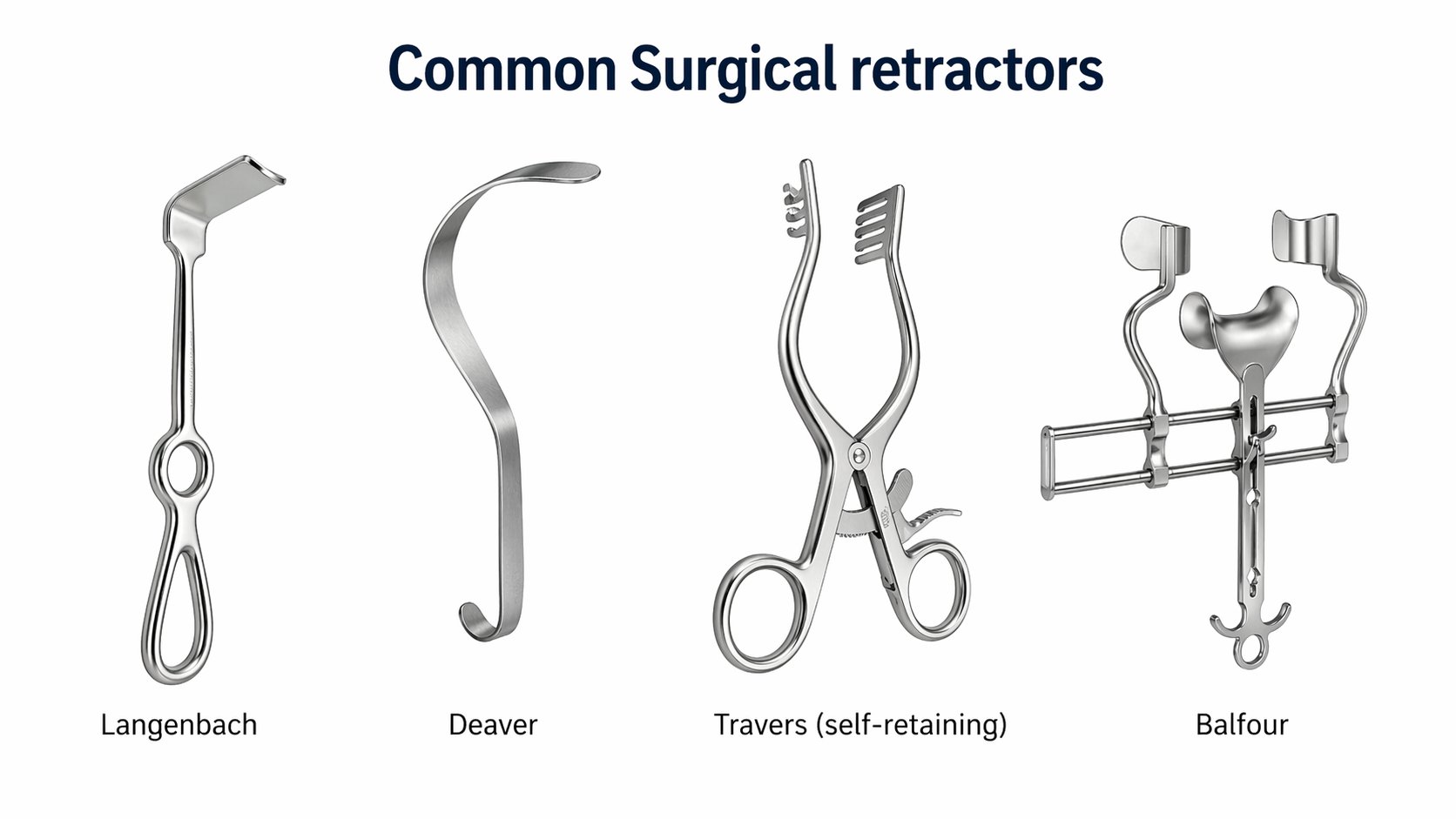
Retractors hold tissue away from the operative field without requiring a hand to hold them (self-retaining) or using a surgical assistant's hand (hand-held). The scrub nurse or assistant manages hand-held retractors throughout a case; choosing the right one is part of planning the operation.
Langenbeck retractor is the standard general-purpose hand-held retractor: a flat blade on an angled handle, available in various widths and depths. Suitable for most open abdominal and superficial procedures.
Deaver retractor has a deep curved blade that provides excellent retraction of the liver edge and other deep abdominal structures. Available in different widths.
Army-Navy retractor is a double-ended hand-held retractor with two blades of different sizes, useful for shallow wound retraction.
Travers self-retaining retractor uses ratcheted arms to hold itself open, allowing hands-free retraction of superficial wounds. Balfour retractor is the standard self-retaining abdominal retractor with a central blade for the bladder and two lateral arms for the abdominal wall. Bookwalter and Thompson retractors are fixed ring-and-blade systems attached to the operating table, providing the most stable retraction for complex abdominal procedures.
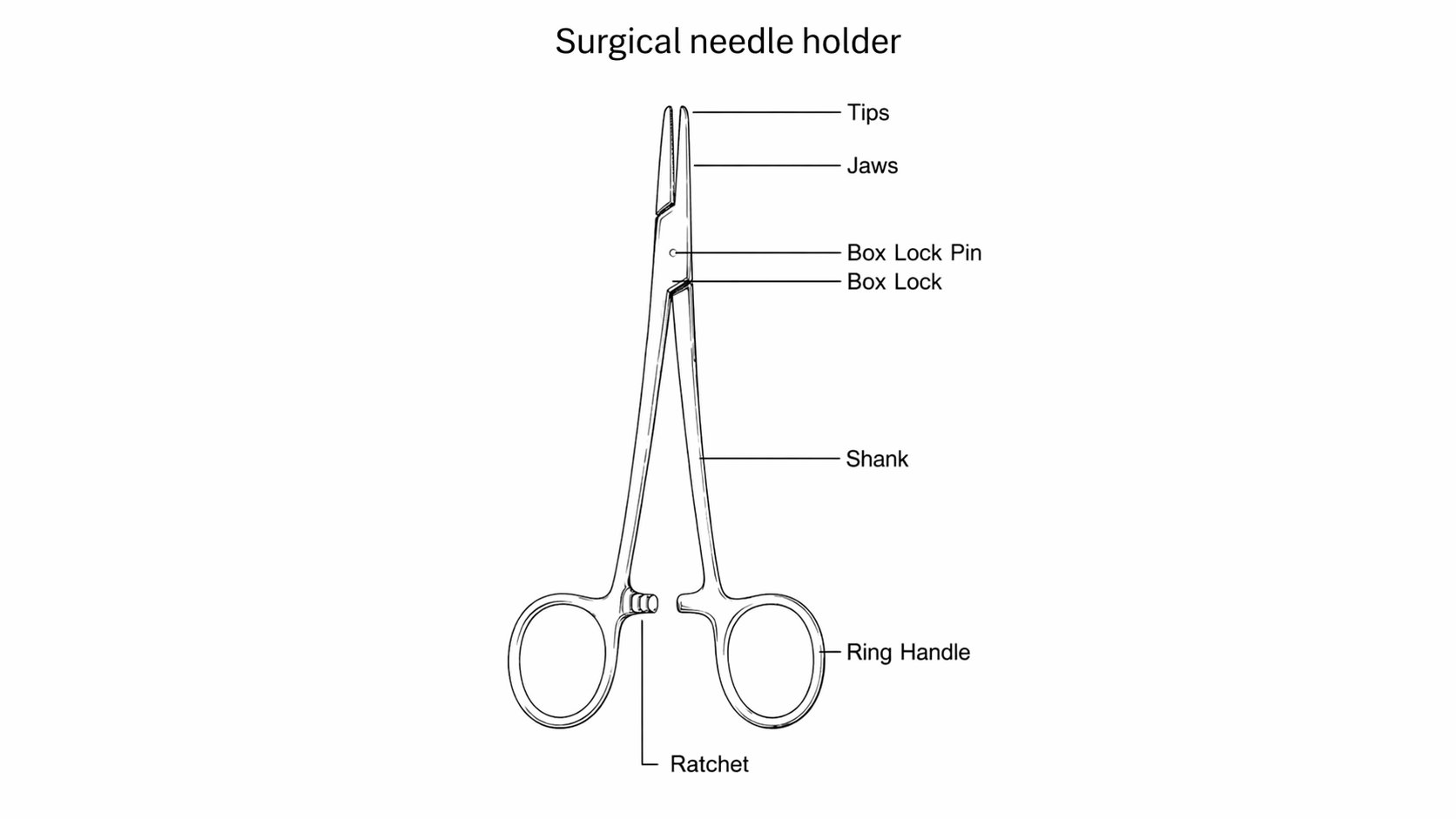
Needle holders are ratcheted instruments with a short, stubby jaw designed to grip a surgical needle securely without deforming it. The jaw surface is hardened, typically with tungsten carbide inserts, which grip the needle without slipping. Tungsten carbide instruments are identified by their gold-coloured handles. Standard needle holders have silver handles with hardened steel jaws that wear more quickly.
The jaw width must be matched to the needle size. A fine needle in a heavy holder will be deformed; a heavy needle in a fine holder will slip. If the needle rotates in the jaws when you apply light pressure, the holder is the wrong size or needs replacing.
Mayo-Hegar needle holder is the standard general-purpose needle holder, available in several lengths. Olsen-Hegar combines a needle holder with integral scissors, allowing suture cutting without instrument exchange. Useful for interrupted suturing but impractical for continuous suturing where frequent cutting would disrupt the rhythm.
Suction keeps the operative field clear of blood and fluid. The choice of suction tip determines how effectively this is achieved.
Yankauer suction tip is a rigid, wide-bore tip used to clear large volumes of fluid rapidly from the abdomen, chest, or pelvis. The standard choice for open abdominal surgery.
Frazier-Ferguson suction tip is a fine, angled tip with a vent hole near the handle. Occluding the vent with a finger activates suction; releasing it stops flow, allowing precise control in delicate dissection or in confined spaces such as the ear canal or skull base.
Poole suction tube is a double-barrel tube with multiple side holes on the outer sheath, designed to prevent omental or bowel plugging when evacuating large volumes from the peritoneal cavity.
Instruments on the trolley follow a strict organisation that the scrub nurse establishes and maintains. Each instrument has a place, and returning instruments to their place after use is the surgeon's responsibility, not just the scrub nurse's. A disorganised trolley slows the operation, increases the risk of sharps injuries, and makes counting harder at closure.
Instruments with ratchets should be handed back with the ratchet open. Scissors and needle holders are handed back with the tips pointing away from the scrub nurse. Sharps, including loaded needle holders and scalpels, are passed via a kidney dish or neutral zone rather than hand to hand.