The skin of your hands carries two populations of bacteria. Resident bacteria are the commensals that live permanently in the hair follicles, sweat glands, and under the nails: organisms such as Staphylococcus epidermidis and, less commonly, Staphylococcus aureus. You cannot eliminate them, but you can suppress them. Transient bacteria are acquired from contact with contaminated surfaces and are more easily removed. Surgical hand antisepsis targets both: mechanical scrubbing removes transient organisms and reduces commensal counts, and chemical antiseptics suppress regrowth during the procedure.
Sterile gloves are worn immediately after to prevent recontamination. They are not a substitute for scrubbing. Gloves develop micro-perforations during use, and the warm moist environment inside a glove allows any residual bacteria to multiply rapidly. A poorly scrubbed hand inside a perforated glove is a significant infection risk.
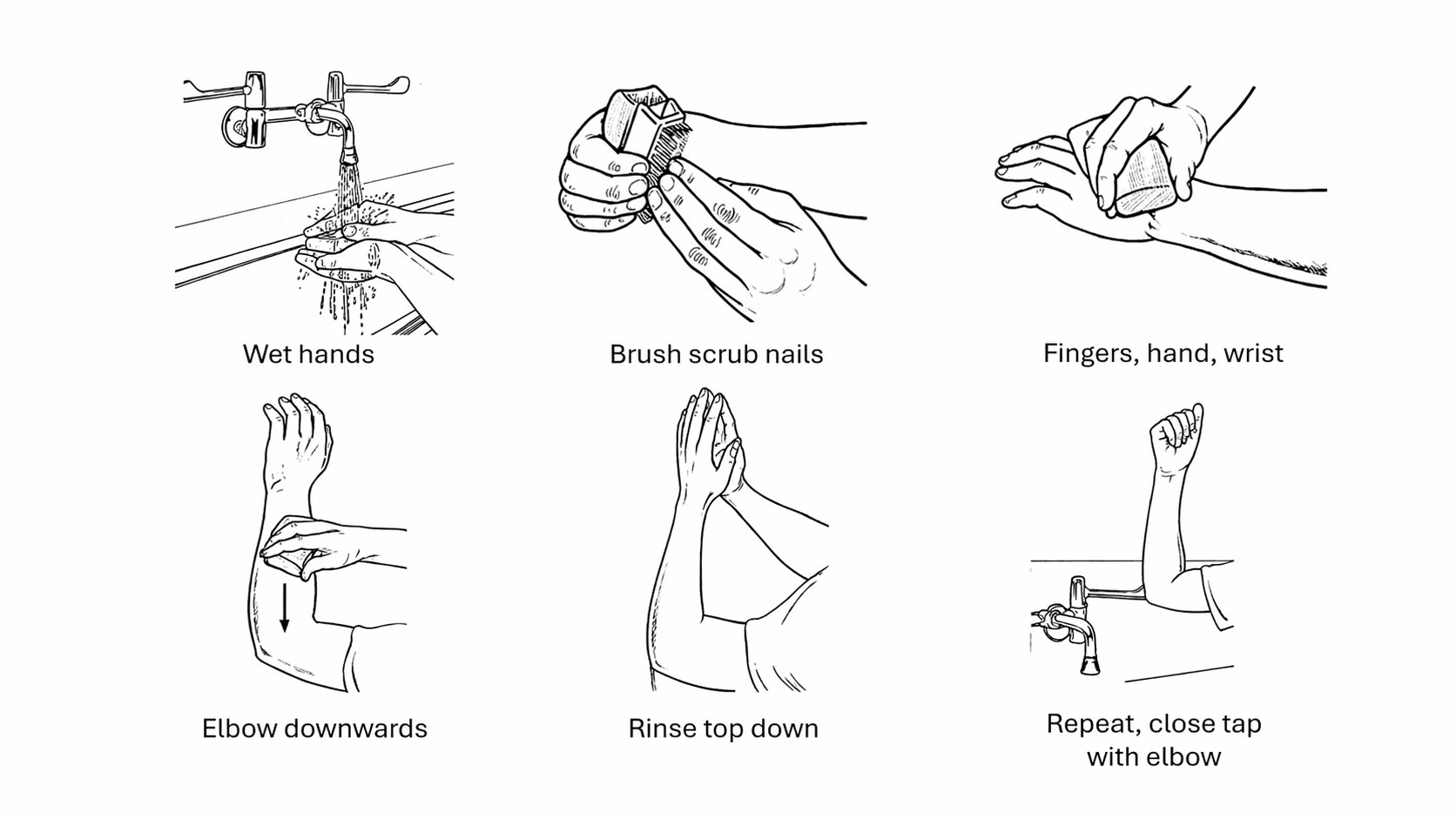
Several checks must be completed before you approach the scrub sink. Anyone with a hand infection, broken skin, or an active upper respiratory infection should not scrub. Remove all hand jewellery including rings, bracelets, and watches. Nail varnish and artificial nails are not permitted. Roll your sleeves to at least four inches above the elbow. Ensure your cap covers all hair and your mask covers nose and mouth completely. If you wear glasses, ensure they fit securely and will not fall into the sterile field.
The antiseptic solution of choice in most UK theatres is 4% chlorhexidine gluconate in a detergent base, which has prolonged residual activity against both gram-positive and gram-negative organisms. Povidone iodine is an alternative. Alcohol-based hand rubs are used in some centres as an adjunct after the initial scrub, applied to thoroughly dried hands and allowed to air dry completely before gowning.
The timed method is the most widely used. The total scrub time is 2 to 6 minutes for the first procedure of the day, following the antiseptic manufacturer's recommendation. Subsequent procedures require a shorter scrub. The old practice of 10-minute scrubs is no longer recommended and causes unnecessary skin damage.
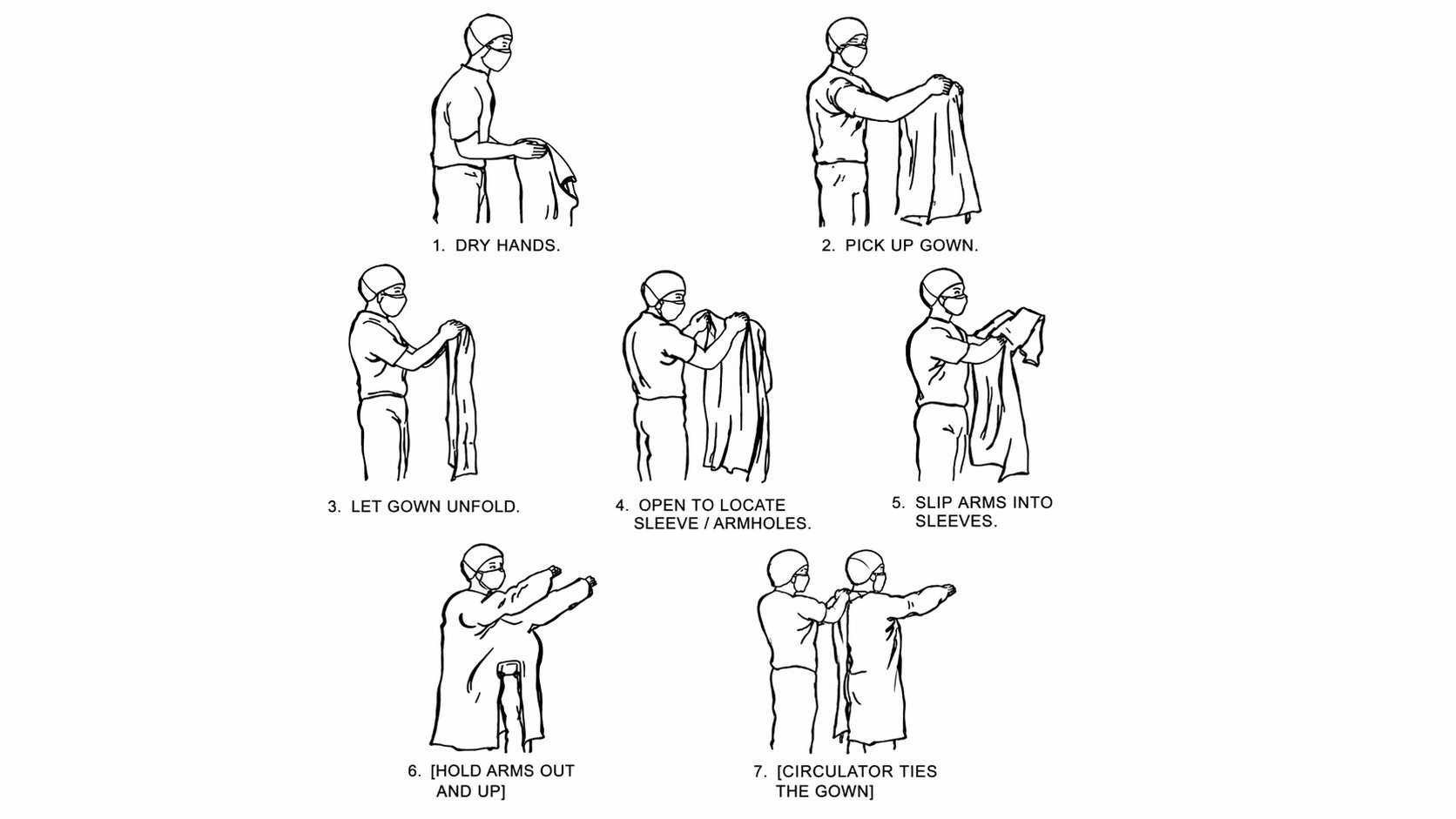
Pick up the sterile towel from the gown pack and step back from the sink. The towel must contact only your scrubbed hands and forearms. Place the unfolded towel on one hand. Using the upper surface, dry the opposite hand and forearm with a blotting motion, working distal to proximal. Turn the towel over and dry the second side. Discard the towel without touching anything further. Apply alcohol rub if required by local policy and allow it to dry completely.
After drying, keep hands and forearms above waist level and held away from your body at roughly 20 to 30 degrees above the elbow. This position must be maintained until you are fully gowned and gloved.
Lift the gown from the wrapper by its neckline, touching only the inner surface. Step back from the table and allow it to unfold gently. Do not shake it. Slip both arms simultaneously into the sleeves and advance your hands toward the cuffs, but do not let your hands emerge through the cuffs. Keeping hands inside the cuffs is essential for closed gloving. The circulating nurse ties the gown at the back without touching your hands or the sterile exterior. Once gloved, the wraparound tie at the front can be secured with the help of the circulator or a scrubbed team member.
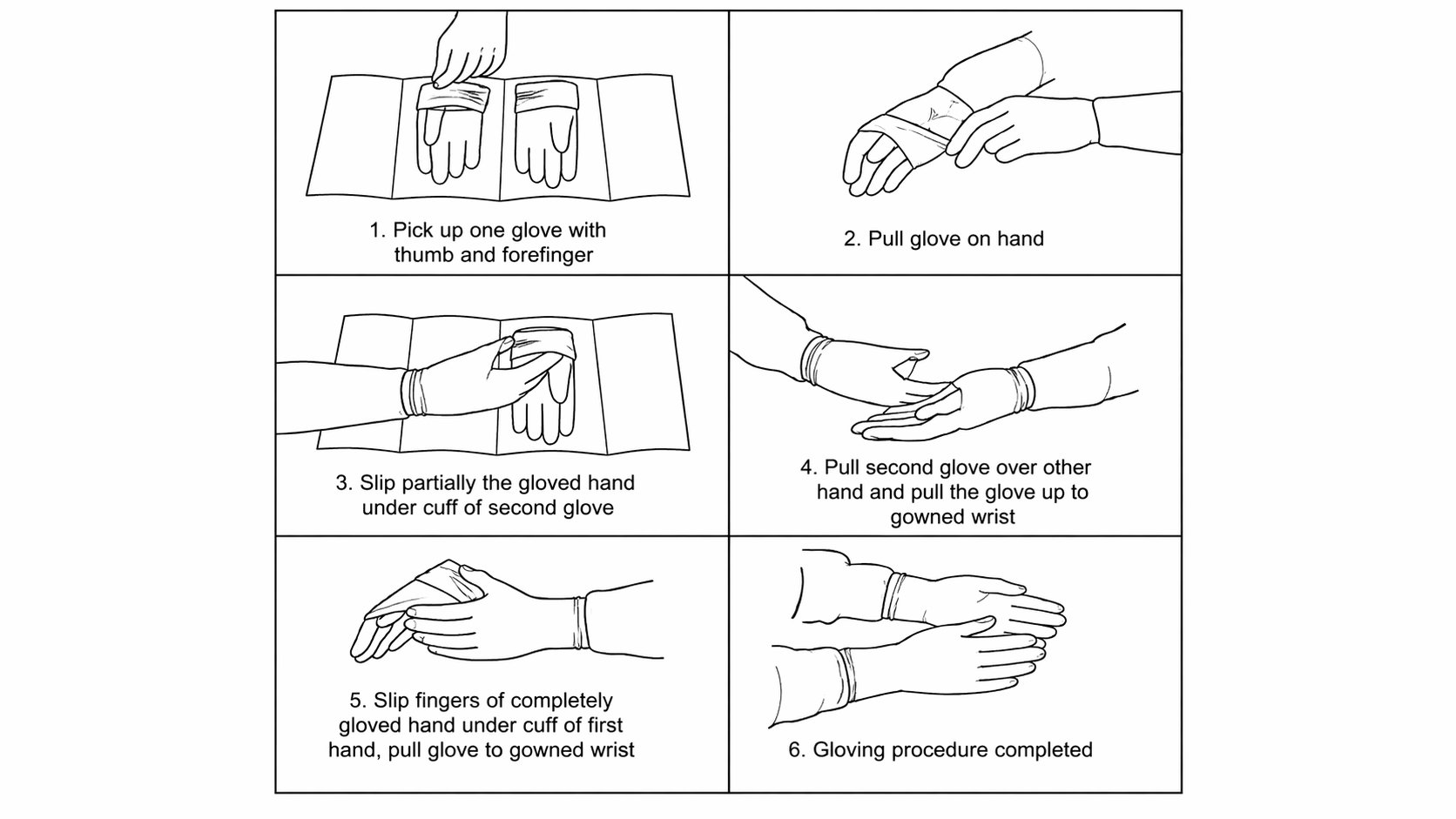
Closed gloving is the standard technique for the initial scrub before a procedure because it ensures no skin contacts the outer surface of the glove. The hands remain inside the gown cuffs throughout.
Left glove: With your right sleeve-covered hand, grasp the cuff of the left glove from the pack. Place it palm-down on the left palm, fingers pointing toward the elbow. Grasp the top edge of the glove cuff with the left hand through the gown, then use the right sleeve-covered hand to pull the glove cuff over the left sleeve cuff, turning it back over the gown. Push the left hand through into the glove, ensuring the gown cuff is covered.
Right glove: The now-gloved left hand can handle the outside of the right glove directly. Place the right glove on the right sleeve in the same orientation, pull the cuff over, and advance the right hand through.
Inspect both gloves for integrity. Any perforation means the glove must be changed before the procedure begins.
Open gloving is used for changing a glove on the operating table when contamination or perforation occurs, and for minor bedside sterile procedures that do not require gowning. In this technique the skin of the hand briefly contacts the inner surface of the glove cuff, which is acceptable because the inner surface is not part of the sterile field. The gloved hand then handles the second glove exclusively by its outer cuff to maintain sterility of the outer surface.
A scrubbed, gowned, and gloved colleague can assist gloving by holding the glove open with fingers under the cuff and thumbs outward, stretching it wide. The person being gloved inserts their hand directly into the open glove. This is the technique used when a second surgeon scrubs in during a procedure.
At the end of a procedure, the gown is removed first by grasping the shoulders, pulling it downward, and turning it inside out as it comes off so the contaminated outer surface is folded inward. Gloves are removed using the glove-to-glove then skin-to-skin technique: grasp the outside cuff of the first glove with the gloved opposite hand and peel it inside out. Slide the bare fingers of the now-ungloved hand inside the second glove cuff and peel it inside out over the first glove. Discard together. Wash hands.